In this post I will continue the discussion on how we incorporate reconditioning aspects into our programs here at Lewis Fitness & Performance. Make sure you check out Part I to get caught up on all of the concepts covered previously. In this post we will look at how reconditioning and athletic development go hand-in-hand, a mind set shift away from the term rehabilitation and return to play being redefined to best prepare the athlete for future success. .
Athletic Development
As a performance-based model, reconditioning is identified more closely with the field of Athletic Development than Sports Therapy. As an Athletic Development professional, I am a part of a performance team whose goal is to train all components of athleticism to the level required by the sport in which the athlete participates. The performance team is comprised of the team physician, therapists, athletic development coaches, nutritionist, sports scientists, performance psychologists and technical sport coaches.
In reconditioning, we need to appreciate that our job is to enhance athleticism, which is the ability to perform athletic movements at optimal speed with precision, and efficiency.4 This means that reconditioning follows that same functional path immediately post Injury or following surgery until the athlete returns to competition. It is a path that explores what an athlete can do as they begin their preparation for more advanced training. In order to prepare for quality movements with precision and style, all treatment decisions following injury greatly matter. If you brace a knee, for example, for 12 weeks following surgery, you can expect a conflict with achieving optimal speed with grace when it matters most. This happens due to the altered mechanics that a brace inflicts on the athlete. But if you were to progressively re-establish neuromuscular control to stabilize the knee (utilizing the body's own intrinsic ‘bracing‘) with properly loaded sport-specific movement patterns, you may actually improve the quality of speed in competition.
As a performance-based model, reconditioning is identified more closely with the field of Athletic Development than Sports Therapy. As an Athletic Development professional, I am a part of a performance team whose goal is to train all components of athleticism to the level required by the sport in which the athlete participates. The performance team is comprised of the team physician, therapists, athletic development coaches, nutritionist, sports scientists, performance psychologists and technical sport coaches.
In reconditioning, we need to appreciate that our job is to enhance athleticism, which is the ability to perform athletic movements at optimal speed with precision, and efficiency.4 This means that reconditioning follows that same functional path immediately post Injury or following surgery until the athlete returns to competition. It is a path that explores what an athlete can do as they begin their preparation for more advanced training. In order to prepare for quality movements with precision and style, all treatment decisions following injury greatly matter. If you brace a knee, for example, for 12 weeks following surgery, you can expect a conflict with achieving optimal speed with grace when it matters most. This happens due to the altered mechanics that a brace inflicts on the athlete. But if you were to progressively re-establish neuromuscular control to stabilize the knee (utilizing the body's own intrinsic ‘bracing‘) with properly loaded sport-specific movement patterns, you may actually improve the quality of speed in competition.

Following the progressive path that reconditioning advocates requires knowledge and experience to understand the movements that transfer to sport performance. The specialist involved in the reconditioning process must have the personality to ‘coach’ the athlete consistently towards improved movement proficiency. The adage that ‘practice does not make perfect; practice makes permanent, ‘should be apparent here. You must coach consistently well or be prepared for compromised performance or potential re-injury in the future. This is imperative to realize that the coaching aspect is the primary factor in reconditioning. As athletes return to the training environment they do so with multiple compensations around injury. Initially this is not the primary concern within the therapy session as inflammation, pain reduction and ROM of the injured joint/muscle are the primary factors. As athletes return to training where the focus shifts to overall athletic function, uncovering and retraining compensation patterns become a focus of training and a qualified fitness professional is needed to assess movement compensation and direct the programming toward correction and ensure safety.
"The goal of the preparation period is to return the athlete to the highest level of training within the shortest period of time while respecting homeostasis, and then staying there for a significant period of time to demonstrate sustainability."
Injury should never interfere with an opportunity to train an athlete. We need to look at ways to train around the injury. Unfortunately, most early and middle-stage rehabilitation protocols are designed to protect the injury by preventing or limiting normal movement patterns. Reconditioning takes an Athletic Development approach during this same stage by encouraging normal movement patterns as soon as possible. This is done in creative ways that protect the injury but always contribute towards re-establishing proper athletic patterns. The brain is extremely plastic; thus every movement pattern that is imparted on the athlete during a post-op period may affect performance. For example allowing an athlete to squat in waist-to-chest-deep water following hip surgery offers a low load functional movement pattern at the ankle, knee and hip that the brain recognizes as segmentally correct movements without pain. This movement on land is often discouraged for many weeks for fear of harming the healing structures; thus it becomes about what you cannot do (as water is not discussed as an option). I feel the less we move correctly, the more harm we may be doing - at many different levels.
Preparation
In a performance-based retraining model, we view post-injury care as a preparation phase rather than a rehabilitation phase. This is a subtle but critical paradigm shift as we are preparing the athlete for a return to competition, not just repairing the injury. The goal of the preparation period is to return the athlete to the highest level of training within the shortest period of time while respecting homeostasis, and then staying there for a significant period of time to demonstrate sustainability. These qualities must be planned starting immediately after injury or surgery to achieve high performance upon their return. Adaptive qualities take time to develop and are dependent on fundamentally sound movement patterns. Too often athletes have ‘adapted’ to the physician’s/therapist’s protocol over months; yet this protocol often underestimates the true demands that team training or competition requires. This is an example where the athlete is not ‘adaptable’ based on the program design and thus cannot sustain high intensity efforts over time.
Return to Competition Phases
The end-stage goal of rehabilitation is commonly referred to as Return to Play (RTP). Yet in performance training, that term is rarely used to describe a phase of preparation or training in an annual plan. Most commonly we discuss training, rest-recovery, competition-competing and performance-performing. The medical community has used the term Return to Play to broadly describe a final rehabilitation phase that represents skill training, team training, scrimmages, games and/ or competition. The RTP stage of a typical rehabilitation protocol usually designed a less structured, under-developed plan to prepare the athlete for high-intensity competitive training or games. This is not surprising, as it is not an area of expertise for traditionally trained medically minded professionals.
The reconditioning model uses the term Return to Competition as it represents a more realistic understanding of the demands that are about to be placed on the athlete. Competition is usually more intense and more demanding on the body than team training or play. In most sports, injury and re-injury happen more often in competition than in training/practice. Therefore, to earn the right to compete you must have progressed successfully through a high-intensity preparation period over time to show your ability to sustain that stress. An experienced athletic development coach who truly understands performance and the demands a particular sport requires must develop this level of program design.
Preparation
In a performance-based retraining model, we view post-injury care as a preparation phase rather than a rehabilitation phase. This is a subtle but critical paradigm shift as we are preparing the athlete for a return to competition, not just repairing the injury. The goal of the preparation period is to return the athlete to the highest level of training within the shortest period of time while respecting homeostasis, and then staying there for a significant period of time to demonstrate sustainability. These qualities must be planned starting immediately after injury or surgery to achieve high performance upon their return. Adaptive qualities take time to develop and are dependent on fundamentally sound movement patterns. Too often athletes have ‘adapted’ to the physician’s/therapist’s protocol over months; yet this protocol often underestimates the true demands that team training or competition requires. This is an example where the athlete is not ‘adaptable’ based on the program design and thus cannot sustain high intensity efforts over time.
Return to Competition Phases
The end-stage goal of rehabilitation is commonly referred to as Return to Play (RTP). Yet in performance training, that term is rarely used to describe a phase of preparation or training in an annual plan. Most commonly we discuss training, rest-recovery, competition-competing and performance-performing. The medical community has used the term Return to Play to broadly describe a final rehabilitation phase that represents skill training, team training, scrimmages, games and/ or competition. The RTP stage of a typical rehabilitation protocol usually designed a less structured, under-developed plan to prepare the athlete for high-intensity competitive training or games. This is not surprising, as it is not an area of expertise for traditionally trained medically minded professionals.
The reconditioning model uses the term Return to Competition as it represents a more realistic understanding of the demands that are about to be placed on the athlete. Competition is usually more intense and more demanding on the body than team training or play. In most sports, injury and re-injury happen more often in competition than in training/practice. Therefore, to earn the right to compete you must have progressed successfully through a high-intensity preparation period over time to show your ability to sustain that stress. An experienced athletic development coach who truly understands performance and the demands a particular sport requires must develop this level of program design.
 | 2 |
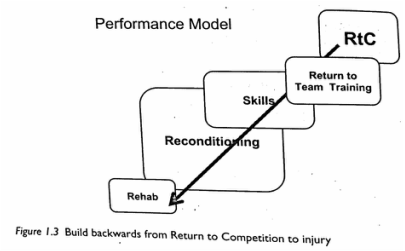
Build backwards: A performance team looks carefully at how the athlete physically needs to look to be competitive and to reduce the risk of injury. It then strategically builds backwards to address the post injury and post-operative plan. This plan is developed with the medical team, but not owned by one particular profession. For example there should be significant contact time with the athletic development staff during all RTC stages. All professions need to work in an interdisciplinary manner to ensure that the athlete is kept safe and healing structures are protected, and that they are skillfully trained in all aspects of athletic competency.
Reconditioning programs are criteria based, not protocol driven. There should be no steadfast timeline that controls the progression an athlete mousse torte a return to training and, ultimately, return to competition. Guideline should be created to monitor homeostatic responses to weekly/monthly training, and biological healing should be respected and monitored as indicated. Movement quality training, strength, coordination, speed and power will address the neurophysiologic dysfunctions that occur with injury, but they must be developed early and often throughout the program. Ultimately, consistent performance team reviews will determine an athlete preparedness for the next level of reconditioning. This is very important to avoid detrimental phases (down-time) in a program where athletes are not allowed to progress and a rate necessary to keep them safe and promote performance.
Reconditioning programs are criteria based, not protocol driven. There should be no steadfast timeline that controls the progression an athlete mousse torte a return to training and, ultimately, return to competition. Guideline should be created to monitor homeostatic responses to weekly/monthly training, and biological healing should be respected and monitored as indicated. Movement quality training, strength, coordination, speed and power will address the neurophysiologic dysfunctions that occur with injury, but they must be developed early and often throughout the program. Ultimately, consistent performance team reviews will determine an athlete preparedness for the next level of reconditioning. This is very important to avoid detrimental phases (down-time) in a program where athletes are not allowed to progress and a rate necessary to keep them safe and promote performance.
1 Gambetta, V. (2007). Athletic Development: The art and science of functional sports conditioning. Champaign, Il: Human Kinetics.
2 Joyce, D., and Lewindon, D. (2016). Sports Injury and Rehabilitation: Integrating Medicine and Science For Performance Solutions. New York, NY: Routledge.
2 Joyce, D., and Lewindon, D. (2016). Sports Injury and Rehabilitation: Integrating Medicine and Science For Performance Solutions. New York, NY: Routledge.

 RSS Feed
RSS Feed